
Myocardial scintigraphy in suspected amyloidosis
A practical guide for referring physicians
Principle and method
 Amyloidosis is a heterogeneous group of diseases characterised by extracellular deposition of fibrillar proteins, leading to progressive organ involvement. Cardiac amyloidosis, particularly transthyretin (ATTR) and AL (light-chain) amyloidosis, is associated with severe cardiomyopathy, heart failure and a poor prognosis.
Amyloidosis is a heterogeneous group of diseases characterised by extracellular deposition of fibrillar proteins, leading to progressive organ involvement. Cardiac amyloidosis, particularly transthyretin (ATTR) and AL (light-chain) amyloidosis, is associated with severe cardiomyopathy, heart failure and a poor prognosis.
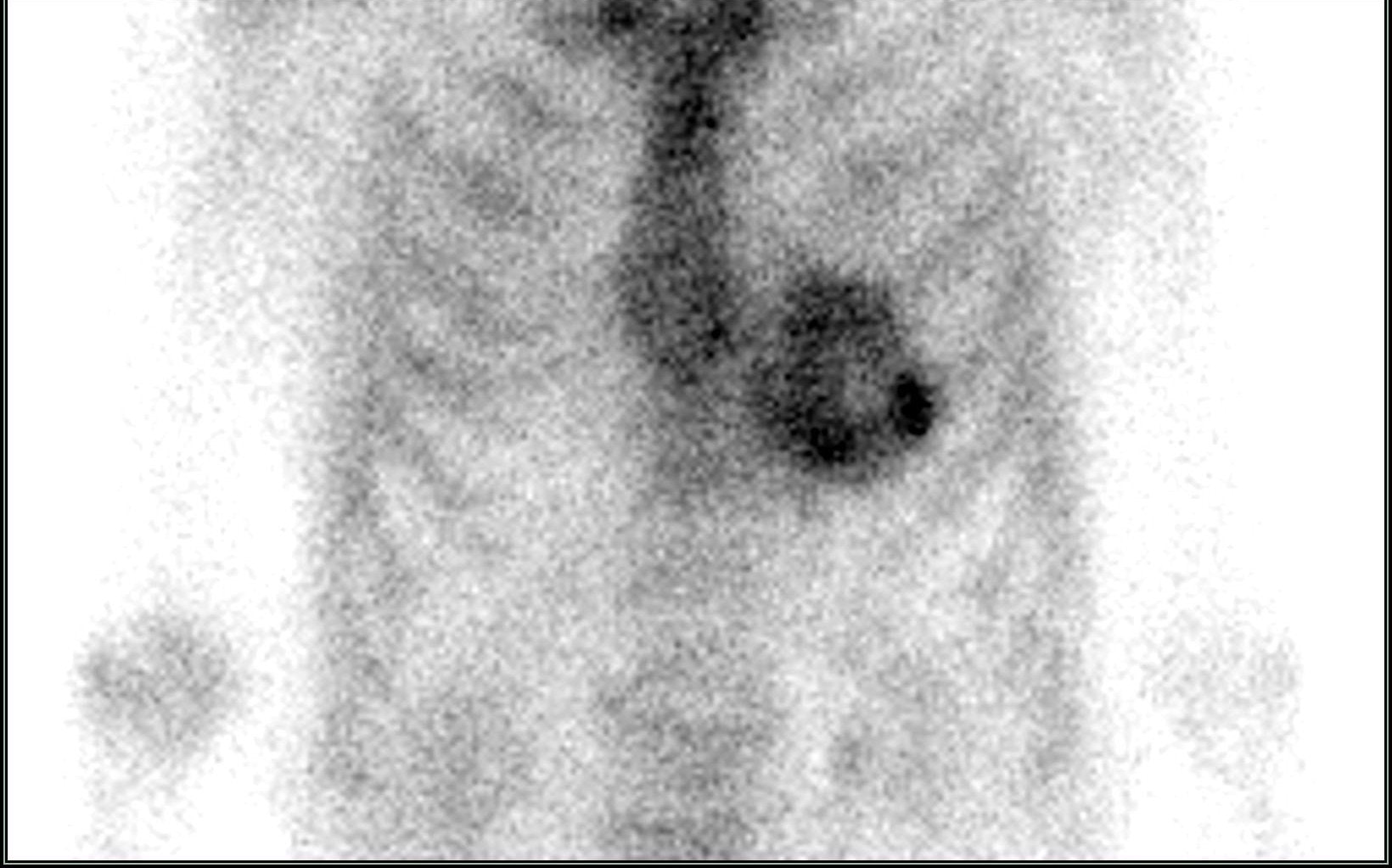
Traditionally, the diagnosis of cardiac amyloidosis has been based on endomyocardial biopsy. In recent years, however, non-invasive diagnosis using phosphonate radiopharmaceutical scintigraphy has become established:
- 99mTc-DPD (3,3-diphosphono-1,2-propanedicarboxylic acid),
- 99mTc-PYP (pyrophosphate),
- 99mTc-HMDP (hydroxymethylenediphosphonate).
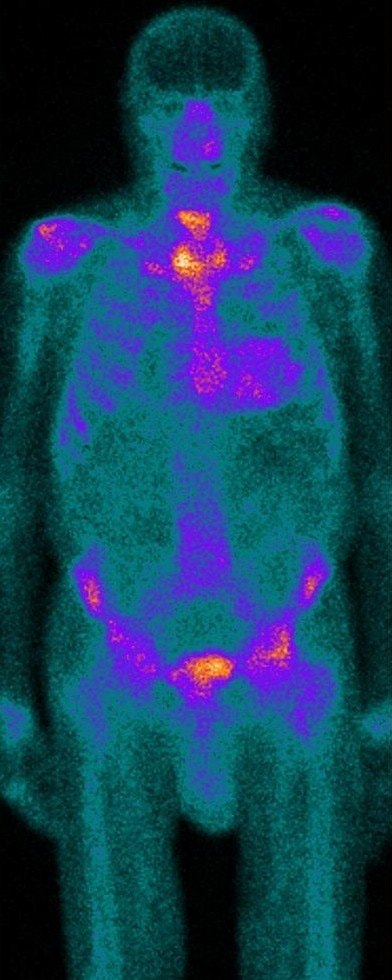 These substances bind to amyloid fibrils in the myocardium and enable specific detection of TTR amyloidosis. Imaging is performed planarly and using SPECT/CT, which provides detailed anatomical and functional information.
These substances bind to amyloid fibrils in the myocardium and enable specific detection of TTR amyloidosis. Imaging is performed planarly and using SPECT/CT, which provides detailed anatomical and functional information.
Main clinical indications
- Suspected cardiac amyloidosis in patients with:
- hypertrophic cardiomyopathy of unclear aetiology,
- restrictive cardiomyopathy,
- heart failure with diastolic dysfunction,
- unexplained left ventricular hypertrophy on echocardiography or MRI.
- Differentiation of types of amyloidosis:
- phosphonate scintigraphy is highly specific for ATTR,
- AL amyloidosis usually does not show significant uptake.
- Prognostic stratification – the extent of accumulation correlates with the severity of the condition and prognosis.
- Monitoring the effect of therapy – especially with new drugs affecting transthyretin (tafamidis, patisiran, inotersen).
Interpretation and clinical significance
Evaluation of findings
- Grade 0: no accumulation in the myocardium.
- Grade 1: minimal uptake less than in the ribs.
- Grade 2: accumulation similar to that in the ribs.
- Grade 3: accumulation higher than in the ribs with clear visualisation of the myocardium.
The difference between ATTR and AL amyloidosis is significant:
- ATTR: typically strong accumulation of radiopharmaceutical.
- AL: mostly negative or only weak uptake.
The combination of scintigraphy with negative immunofixation testing of serum and urine allows for non-invasive confirmation of ATTR amyloidosis without the need for a biopsy.
Practical information for the referring physician
- Patient preparation: no special diet or discontinuation of medication is necessary.
- Examination procedure:
- intravenous administration of 99mTc-phosphonate,
- planar images of the heart and entire body approximately 1–3 hours after administration,
- supplemented by SPECT/CT for a more accurate assessment of accumulation and differentiation from bone activity.
- Examination duration: 2–3 hours.
- Contraindications: pregnancy; relative contraindication in breastfeeding women.
Summary for practice
Myocardial scintigraphy with phosphonate radiopharmaceuticals is:
- a key method for diagnosing TTR amyloidosis,
- capable of distinguishing TTR from AL amyloidosis in a non-invasive manner,
- essential for early diagnosis and initiation of targeted therapy,
- a safe, accessible and prognostically significant method.
Its introduction has fundamentally changed the approach to the diagnosis of cardiac amyloidosis – it allows for rapid and reliable diagnosis without the need for invasive biopsy, thereby improving patient care and prognosis.
